7. Key concepts underpinning the NOCC protocol¶
Under the NOCC protocols the required data is collected at key Collection Occasions within an Episode of Mental Health Care provided by a Mental Health Service Organisation within a specific Episode Service Setting. The specific clinical measures and other data elements that should or may be collected at any given Collection Occasion are determined by the Episode Service Setting within which the occasion occurs, the Collection Age Group to which the patient or client has been assigned, and whether the Collection Occasion itself is defined as an Admission, a Review or a Discharge.
The key concepts: Episode of Mental Health Care; Episode Service Setting; Collection Occasion; Collection Age Group; and Mental Health Service Provider Entity are each discussed in detail below.
7.1. Episodes of Mental Health Care¶
7.1.1. Concepts of episodes are used widely throughout the health system as a convenient method to describe the activities of health services and to organise data collection, reporting and analysis. In general, an episode of care is used to refer to a period of care with discrete start and end points.
7.1.2. Most work on defining episodes has been tied to acute hospital settings, where the principle is relatively simple – one episode per patient per hospital at any one time, with the episode beginning at admission and ending at discharge.
7.1.3. In the original planning for introduction of NOCC, significant problems arose when translating this concept to community-based mental health services. No concept of episode had been agreed to quantify these types of services. There are several issues that make the definition of an episode in that setting particularly difficult. First, whilst the initiation of community–based mental health care is usually accompanied by formal well–defined processes, its termination often is more difficult to define, either clinically or administratively. Second, many patients undergo care over extended periods. Finally, multiple agencies or teams, working in either the same or different service settings, may be involved in providing care during a particular period, with each agency or team regarding their intervention as a discrete episode.
7.1.4. For the purposes of the NOCC specification, an Episode of Mental Health Care is defined as a more or less continuous period of contact between a consumer [1] and a Mental Health Service Organisation that occurs within the one Episode Service Setting.
7.1.5. This formal concept of an episode should not be confused with either the clinical concept of an episode of care or the more narrowly defined, inpatient- centred definition currently used in the National Health Data Dictionary.
7.1.6. Three broad episode types are identified which are based on the Episode Service Setting – Psychiatric Inpatient, Community Residential and Ambulatory.
- Psychiatric Inpatient episodes (Overnight admitted) – refers to the period of care provided to a consumer who is admitted for overnight care to a public sector specialised psychiatric inpatient service.
- Community Residential episodes – refers to the period of care provided to a consumer who is admitted for overnight care to a public sector specialised community-based residential service.
- Ambulatory episodes – refers to all other types of care provided to consumers of a public sector specialised community-based ambulatory mental health service.
Note that Psychiatric inpatient episodes’ as defined for the purpose of the NOCC protocol are confined to the category of overnight admitted patients as used in the National Health Data Dictionary and specifically exclude same day admitted patients. Same day admitted patient episodes, which account for approximately one quarter of all separations from public sector psychiatric inpatient units, are defined as occasions of service within Ambulatory care episodes for NOCC purposes. This is consistent with the reporting practices that have been in place for the National Survey of Mental Health Services since 1994, and its successor, the NMDS – Mental Health Establishments.
7.1.7. Two business rules apply to episodes of mental health care:
- One episode at a time: While an individual may have multiple episodes of mental health care over the course of their illness, they may be considered as being in only one episode at any given point of time for a particular Mental Health Service Organisation. The practical implication is that the care provided by a Mental Health Service Organisation to an individual consumer at any point in time is subject to only one set of reporting requirements. Where a person might be considered as receiving concurrently two or more episodes of mental health care by virtue of being treated by the organisation in more than one setting simultaneously, the following order of precedence applies: Inpatient, Community Residential, Ambulatory. [2]
- Change of setting = new episode: A new episode is deemed to commence when a person’s care is transferred between inpatient, community residential and ambulatory settings. A change of Episode Service Setting therefore marks the end of one episode and the beginning of another.
7.2. Episode Service Setting¶
7.2.1. The Episode Service Setting is the setting within which the Episode of Mental Health Care takes place, as defined by the domain specified in the following clauses.
7.2.2. Psychiatric inpatient service. This setting includes overnight care provided in public psychiatric hospitals and designated psychiatric units in public acute hospitals. Psychiatric hospitals are establishments devoted primarily to the treatment and care of admitted patients with psychiatric, mental or behavioural disorders. Designated psychiatric units in a public acute hospital are staffed by health professionals with specialist mental health qualifications or training and have as their principal function the treatment and care of patients affected by mental disorder. For the purposes of NOCC specification, care provided by an Ambulatory mental health service team to a person admitted to a designated Special Care Suite or ‘Rooming-In’ facility within a community general hospital for treatment of a mental or behavioural disorder is also included under this setting.
7.2.3. Community residential mental health service. A residential mental health service is a specialised mental health service that:
- employs mental health-trained staff on site;
- provides rehabilitation, treatment or extended care;
- to residents provided with care intended to be on an overnight basis;
- in a domestic-like environment; and
- encourages the resident to take responsibility for their daily living activities.
These services include those that employ mental health trained staff on-site 24 hours per day and other services with less intensive staffing. However all these services employ on-site mental health trained staff for some part of each day.
For non-24 hour staffed services to be included in NOCC data reporting, they must employ mental health trained staff on-site at least 50 hours per week with at least 6 hours staffing on any single day. This is consistent with the scope of the NMDS – Residential Mental Health Care.
7.2.4. Ambulatory care mental health service. This setting includes all non–admitted, non–residential services provided by health professionals with specialist mental health qualifications or training. Ambulatory mental health services include community–based crisis assessment and treatment teams, day programs, psychiatric outpatient clinics provided by either hospital or community–based services, child and adolescent outpatient and community teams, social and living skills programs, psychogeriatric assessment services and so forth. For the purposes of the NOCC protocol, care provided by hospital–based consultation–liaison services to admitted patients in non– psychiatric and hospital emergency settings is also included under this setting.
7.3. Collection Occasion¶
7.3.1. A Collection Occasion is defined as an occasion during an Episode of Mental Health Care when the required dataset is to be collected in accordance with a standard protocol. The broad rule is that collection of data is required at both episode start and episode end.
7.3.2. In many cases, the beginning and end of episodes is marked by some objective event such as admission or discharge from hospital or completion of community treatment. However, because episodes may extend over prolonged periods, outcomes and casemix data need to be collected at regular review points during that care, in order to monitor progress and determine if the consumer’s condition has changed during the defined period.
7.3.3. For the purposes of the specification, the maximum interval between collection occasions is based on the standard review period of three months (91 days) as required under the National Standards for Mental Health Services.
7.3.4. Based on the above, three Collection Occasions are identified within an episode when the required data are to be collected:
- Admission to mental health care episode [3] – this refers to the beginning of an inpatient, ambulatory or community residential Episode of Mental Health Care. For the purposes of the NOCC protocol, episodes may start for a number of reasons. These include, for example, a new referral to community care, admission to an inpatient unit, transfer of care from an inpatient unit to a community team and so forth. Regardless of the reason, admission to a new episode acts as the ‘trigger’ for a specific set of data to be collected.
- Discharge from mental health care episode [4] – this refers to the end of an inpatient, ambulatory or community residential Episode of Mental Health Care. As per Admission, episodes may end for a number of reasons such as discharge from an inpatient unit, case closure of a consumer’s community care, admission to hospital of a consumer previously under community care. Regardless of the reason, the end of an episode acts as a ‘trigger’ for a specific set of data to be collected.
- 3 month (91-day) Review of mental health care episode – this refers to the point at which the consumer has been under 13 weeks of continuous care since Admission to the episode, or 13 weeks has passed since the last Review was conducted during the current episode.
7.3.5. Specification of 3-monthly (91 day) reviews as the minimum requirement for consumers under ongoing care is not intended to restrict Reviews that may be conducted at shorter intervals. Such Reviews of a consumer’s status may occur for a number of reasons including, for example:
- in response to critical clinical events or changes in the consumer’s status;
- in response to a change from voluntary to involuntary status or vice versa;
- following a transfer of care between community teams or change of case manager;
- transfers between inpatient wards within a multi-ward hospital;
- compliance with local agency or State-level requirements such as reviews conducted at the 35 day point within inpatient units;
- consumer or carer-requested reviews; and
- other situations where a review may be indicated.
7.3.6. Where an ad hoc Review is conducted for any of the above reasons, it will also be deemed a Collection Occasion and included in the data reported. Such ad hoc Reviews move forward the next due Collection Occasion to 3 months (91 days) subsequently, or Discharge, whichever occurs sooner.
7.3.7. Fig. 7.1 summarises the data collection points under various episode scenarios.
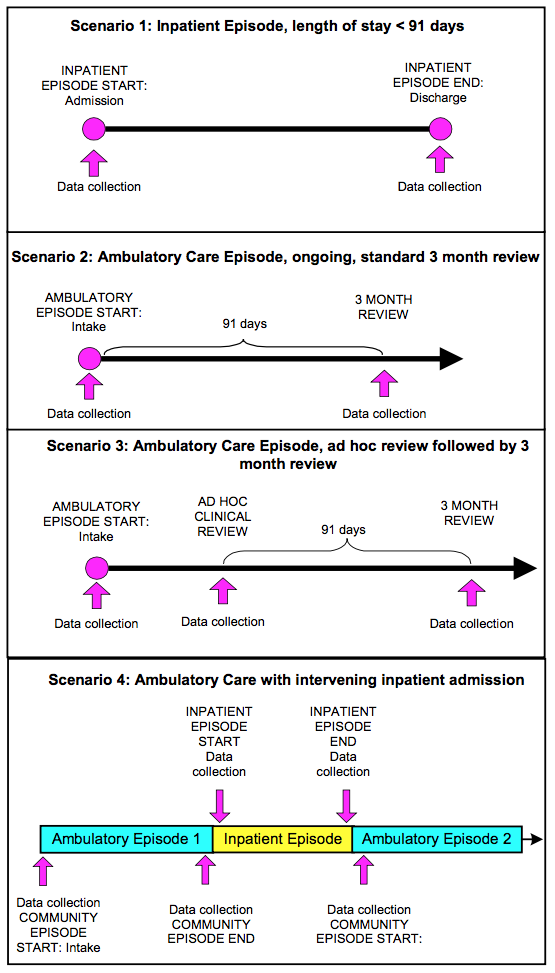
Fig. 7.1 Data collection requirements under four episode scenarios
7.4. Age Group¶
7.4.1. The specific clinical measures to be reported at a particular Collection Occasion depend on the broad age group to which the consumer is assigned (Child and Adolescent, Adult, or Older Persons).
7.4.2. Generally, throughout mental health services, Adults are defined as persons between the age of 18 and 64 years inclusive, Older Persons are defined as persons aged 65 years and older and Children and Adolescents are defined as persons under the age of 18 years.
7.4.3. States and Territories will be responsible for determining whether Age Group (and thus the clinical measures to be used) is determined on the basis of the actual age, condition and care needs of the consumer or deemed on the basis of the type of service providing the treatment and care, or a mixture of both. Currently, all mental health services in-scope are required under the NMDS – Mental Health Establishments to be classified according to the age group of their target population (Child and Adolescent, Older Persons, Forensic, General, Youth). Selection of the clinical measures to be applied by a given service can be based on this service classification.
7.4.4. Thus, in some circumstances a person may be assigned to a different Age Group to that in which they would be assigned on the basis of their actual age, condition and care needs. For example, a person aged 60 years who was being cared for in a specialist Older Persons inpatient unit may be assigned to the Older Persons age group. Similarly, a 15 year old admitted to a general adult psychiatric unit may be assigned to the Adult group if the adult measures are used.
7.4.5. The alternative option of determining which clinical measures to apply on the basis of the consumer’s actual age, condition and care needs has more complex workforce training implications which can only be resolved at the State and Territory level.
7.4.6. Special issues arise in relation to Forensic Psychiatry Services, which may cover all age groups and require additional measures to assessing outcomes. Future national developments in mental health outcome measures will consider options for introducing an agreed set of supplementary measures for Forensic Psychiatry services. In the meantime, each jurisdiction will continue to determine how the concept of Age Group will be interpreted for the Forensic Psychiatry services operating within its public sector.
7.5. Mental Health Provider Entity Hierarchy¶
7.5.1. A systematic approach to the identification of the Mental Health Provider Entity is essential for several reasons:
7.5.1.1 It allows the organisational and service provider contexts in which data are collected to be described. Understanding these service provider contexts is essential for identifying ‘like with like’ services and using the data for benchmarking purposes.
7.5.1.2 When used in combination with the Patient Identifier (see Unique identification of consumers below), it provides the means to:
- assemble data collected at one or more Collection Occasions for a given consumer into higher-level Episodes of Mental Health Care which will be the subject of analysis and reporting; and
- link the outcomes and casemix data provided through the NOCC dataset to unit record data provided by States and Territories collected under related national data sets, in particular, the NMDS – Admitted Patient Mental Health Care, NMDS – Community Mental Health Care and NMDS – Residential Mental Health Care.
7.5.2. Additionally, a systematic approach to the specification of the Mental Health Provider Entity is critical because it determines two aspects of the NOCC protocol:
- It provides the basis for setting the boundaries for how the ‘one episode at a time’ rule is applied. For example, where two ambulatory care teams within a single organisation share responsibility for the care of a consumer, under NOCC this is not considered two separate episodes because both teams (or service units) belong to a single organisation.
- It determines the level at which the consumer is identified uniquely (see Unique identification of consumers below).
7.5.3. Complex issues are raised in designing a system to identify and classify mental health service providers. Services have diversified following the extensive structural reforms under the National Mental Health Strategy. Provider organisations typically provide an array of interlocking services through a number of discrete ‘service units’ or teams which include inpatient units, community-based residential facilities, hospital and community-based outpatient services and mobile assessment and treatment services. The clinical pathways between the various units are also complex. Patients may sometimes be transferred between inpatient facilities, depending on the intensity of care they require. Clients may receive care from more than one ambulatory service within the organisation at the same time, or be transferred between ambulatory care teams for more intensive care for short periods as their needs change.
7.5.4. An additional requirement is that the manner and level at which the responsible Mental Health Provider Entity is specified must enable the meaningful linkage of NOCC data with the unit record data provided by States and Territories under the relevant related NMDS arrangements.
7.5.5. A hierarchical approach is required to deal with this complexity in which the following levels are identified:
- State
- Region
- Mental Health Service Organisation
- Hospital or Service Unit Cluster
- Service Unit
7.5.6. This ‘layered’ approach to the identification of mental health entities developed originally from the National Survey of Mental Health Services that ran between 1994 and 2005, and has been introduced as a central feature of all National Minimum Data Sets. It has proved its worth as an approach to dealing with the complexity of the mental health service system.
7.5.7. In this approach, States and Territories report data aggregated around the concept of a Mental Health Service Organisation and further specify data relating to the various inpatient, ambulatory care and community residential service units that operate beneath the level of the ‘parent’ organisation. All mental health service organisations are in turn grouped into regions.
Specification
7.5.8. Each Collection Occasion record reported as part of the NOCC extract should be assigned to a Service Unit, which is identified by a unique Service Unit Identifier.
7.5.9. Service Units represent the lowest level component of a hierarchically ordered set of entities, comprising five levels within the mental health service system:
- State or Territory
- Region
- Mental health service organisation
- Hospital or Service unit cluster
- Service unit
7.5.10. State or Territory. This level refers to the state or territory and should be reported using the Australian state or territory identifier data element.
7.5.11. Region. The region refers to an administrative concept and is the same as the region concept in the NMDS – Mental Health Establishments. States and Territories may have one or more regions into which the jurisdiction is divided and to which its mental health service organisations belong. In those cases, Region should be reported using the Region data element. In the smaller states or in the territories there may only be one or no region applicable. In these cases the Region code would be reported as ‘00’ and the Region details would repeat the name of the State or Territory.
7.5.12. Mental Health Service Organisation. As defined and described under The definition of a Mental Health Service Organisation. Identifiers used to report Mental Health Service Organisations within NOCC should be the same as those used to identify organisations in the NMDS – Mental Health Establishments.
7.5.13. Hospital or Service Unit Cluster. A mental health service organisation may consist of one or more clusters of service units providing services in admitted patient, residential and ambulatory settings. For example, a mental health service organisation may consist of several hospitals (clusters of admitted patient service units) and/or ambulatory or residential service unit clusters (for example, a cluster of child and adolescent ambulatory service units, and a cluster of aged residential service units).
To allow service units (as defined below using agreed data elements) to be individually identified, but still also to be identified as part of a hospital (for the admitted patient service setting), or as part of another type of cluster (e.g., other cluster types for ambulatory or residential service setting), a separate reporting level called ‘Hospital’ for admitted patient service units and ‘Service unit cluster’ for ambulatory service units and residential service units is necessary.
While all admitted patient service units must be physically part of a hospital, ambulatory and residential service units will not necessarily be part of a natural cluster. However, for some ambulatory service units, the service unit may ‘belong’ to a hospital that contains both admitted patient and ambulatory service units. In this instance, the service unit cluster identifier for the ambulatory service unit would be the ‘hospital identifier’. Other groups of ambulatory and residential service units could also be usefully identified as clusters. For example, clusters may exist of groups of residential services for aged persons, or groups of ambulatory service units in particular geographical areas.
When there is no Service unit cluster, then the Service unit cluster identifier is to be reported as ‘00000’ and the Service unit cluster details would use the relevant organisation name.
Note that hospitals are to be reported as the equivalent of service unit clusters rather than as service units.
7.5.14. Service Unit. The Service Unit represents the lowest level in the Mental Health Provider Entity Hierarchy but is the most critical because it is the level at which patient care is delivered. Three ‘service unit types’ are identified, comprising:
- Psychiatric inpatient (admitted patient) service units
- Residential service units
- Ambulatory service units
7.5.15. Service Unit Type is intended to describe the most common type of care provided by the service unit. Service Unit Type should not be confused with Episode Service Setting. As described below, the latter is an attribute of the Episode of Mental Health Care, while the former is an attribute of the service provider.
7.5.16. Several guidelines apply to the way in which an organisation’s mental health services are reported as service units. These are based on the minimum reporting that is required for the purposes of the National Minimum Data Sets, particularly the NMDS – Mental Health Establishments.
7.5.16.1. Admitted patient service units: Admitted patient service units should be differentiated by Target Population (Child and Adolescent, Older Persons, Forensic, General, Youth) and Program Type (Acute vs Other). For example, if a hospital had separate wards for Child & Adolescent and General Adult populations, these should be reported as separate service units. Similarly, if the hospital provided separate wards for Older Persons acute and Older Person other program types, this would require separate service units to be identified (that is, defined by the program type as well as the target population). The overarching principle is that the same service unit identification policy must be applied to the admitted patient service units data reported under NOCC and the NMDS – Mental Health Establishments.
7.5.16.2. Residential service units: Residential service units should be differentiated by Target Population (Child and Adolescent, Older Persons, Forensic, General, Youth). Where possible, it is also desirable that residential service units identified in NOCC data correspond directly on one-to-one basis to those reported in the NMDS – Residential Mental Health Care.
7.5.16.3. Ambulatory service units: Ambulatory service units should be differentiated by Target Population (Child and Adolescent, Older Persons, Forensic, General, Youth). Where an organisation provides multiple teams serving the same target population, these may be grouped and reported as a single Service Unit, or identified as individual Service Units in their own right. Where possible, it is also desirable that ambulatory service units identified in NOCC data correspond directly on one-to-one basis to those reported in the NMDS – Community Mental Health Care.
7.5.17. When assigning a Service Unit to a Collection Occasion, the following overarching reporting rule applies: Identify the Service Unit that is principally responsible for provision of services to the person during the current episode of care.
7.5.18. Two implications follow from this overarching rule.
7.5.18.1. The Service Unit Identifier recorded for any given Collection Occasion will not necessarily refer to the Service Unit that collected the Collection Occasion data. For example, where an ambulatory care service assists in the admission to hospital of a consumer and completes the required data items and standard measures, the Service Unit Identifier recorded for that Collection Occasion should refer to the admitted patient services unit, not the ambulatory care service unit.
7.5.18.2. The setting reported for the Service Unit (at the data element ‘service unit type’) will not necessarily match the Episode Service Setting within which the Episode of Care takes place as reported at the Collection Occasion level. For example, this could occur where an inpatient service is primarily responsible for providing the services to a person in an ambulatory episode following discharge from hospital.
7.5.19. While the NOCC specifications need to recognise that complex interactions can occur between service type and episode type, in the vast majority of instances the following simple situations will apply.
- Where the collection occasion occurs in the context of an inpatient episode, the Service Unit identified will be the admitted patient service unit within the hospital to which the patient is currently admitted.
- Where the collection occasion occurs in the context of a community residential episode, the Service Unit identified will be the community residential facility to which the patient is admitted.
- Where the collection occasion occurs in the context of an ambulatory episode, the Service Unit identified will generally be the single ambulatory care service that is providing the treatment and care to the person during the episode.
7.5.20. The ‘one episode at a time’ business rule should be applied across the Mental Health Service Organisation not at the Service Unit level. Thus, where multiple Service Units within the organisation are simultaneously involved in providing treatment and care to a consumer, that consumer is considered as receiving only one Episode of Mental Health Care using the order of precedence described in clause 5.1.7. A consumer may however be regarded as receiving more than one episode of care when each episode is provided by a separate Mental Health Service Organisation.
7.5.21. The hierarchical relationship between the components of the Mental Health Provider Entity Hierarchy and the levels at which key NOCC business rules are applied is summarised in Fig. 7.2.
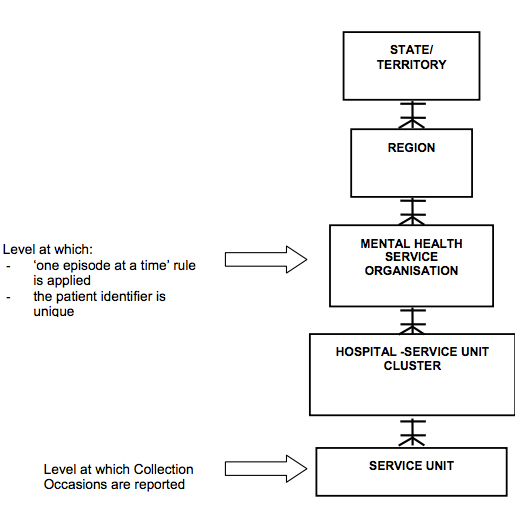
Fig. 7.2 Mental Health Provider Entity Hierarchy – Elements and levels
7.6. Unique identification of consumers¶
7.6.1 Unique identification of the consumer is an essential requirement in clinical information systems, both for ensuring that local information collections support continuity of care, as well as for State/Territory and national-level analysis.
7.6.2. All unit record data reported by States and Territories is to be assigned to an individual consumer, identified by a numerical Patient identifier that is unique at the level of the Mental Health Service Organisation and shared by all service units operating under the organisation.
7.6.3. States and Territories vary in the extent to which service units operating as components of a Mental Health Service Organisation share a unique identifier for patients under care. However, where these are not in place, States and Territories are taking steps to establish such arrangements.
7.6.4. The unique Patient identifier reported in the NOCC extract submitted to the Australian Government should be in encrypted form and meet two fundamental requirements:
- It should be identical to the identifier used in supplying unit record data in respect of the individual consumer in the corresponding NMDS dataset. Thus:
- For consumers reported in the NOCC data set as currently experiencing an ambulatory care episode, the patient identifier used should be identical to that used to supply data in respect of the consumer to the NMDS – Community Mental Health Care.
- For consumers reported in the NOCC data set as currently experiencing a residential care episode, the patient identifier used should be identical to that used to supply data in respect of the consumer to the NMDS – Residential Mental Health Care.
- For consumers reported in the NOCC data set as currently experiencing a psychiatric inpatient episode, the patient identifier used should be identical to that used to supply data in respect of the consumer to the NMDS – Admitted Patient Mental Health Care.
- The encrypted identifier used to supply data to NOCC in respect a consumer should be stable over time – that is, it should allow the consumer’s data to be linked across reporting years.
| [1] | For the purposes of these specifications, the terms consumer, client and patient are used interchangeably and refer to a person for whom a Mental Health Service Organisation accepts responsibility for assessment and/or treatment as evidenced by the existence of a medical record. |
| [2] | The ‘one episode at a time’ rule is an important administrative device to facilitate data collection and development of business rules that clarify ‘what should happen when’. It is not intended to undermine the important concept of continuity of care in mental health service delivery, nor to imply segregation in the service delivery roles of clinical staff working across inpatient and community-based settings. |
| [3] | ‘Admission’ and ‘Discharge’ are used as abbreviated generic terms throughout this document to refer to entry to or exit from care in all treatment settings. While it is recognised that for some mental health clinicians and consumers the terms are not ‘community friendly’, they are used here as economical ways of describing similar events in the cycle of mental health care. Alternative terms for Admission and Discharge are ‘Episode Start’ and ‘Episode End’ or ‘Entry to Episode’ and ‘Exit from Episode’, respectively. |
| [4] | ‘Discharge’ is not formally defined in the National Health Data Dictionary, which uses instead the term ‘separation’ defined as ‘the process by which an episode of care for an admitted patient ceases.’ The NOCC protocol uses the term ‘discharge’ by preference as a generic term to cover the completion of episodes across all treatment settings. |