9. Collection protocol¶
This section describes the protocol to be used to guide the collection of outcomes and casemix data. It focuses on what data is to be collected and when it is to be collected.
The NOCC protocol defines the minimum requirements and should not be interpreted as confining participating States and Territories to those requirements. Additionally, local services may elect to collect additional measures or to increase the frequency of ratings.
Implementing the protocol within service delivery agencies requires consideration of how the required data collection will be integrated within agency-level clinical processes and broader information requirements. Local systems vary with different business processes, data collection forms and so forth that reflect differences in service delivery structures. Resolving these issues is beyond the scope of the current document but will need to be addressed by all States and Territories.
It is important to minimise the burden of collection, where possible, while preserving episodes of care as the fundamental building block of NOCC. The collection protocol as defined in this version builds on the experience of NOCC implementation since 2003. In particular, a wide range of users was consulted throughout the course of the NOCC Strategic Directions 2014-2024 project which has led to some revision of the protocol as implemented in earlier versions of the NOCC Technical Specifications.
9.1. Data requirements at each Collection Occasion¶
9.1.1. Design of the protocol needs to accommodate both the outcomes and casemix development objectives of the agreed information development strategy. These are not identical. Simply put, casemix requirements need key data to be collected only once during each episode to allow the episode to be adequately described and classified. From the casemix perspective, the only issue is to ensure that the information is collected at the most appropriate point within the overall episode of care. For example, assessment on the HoNOS at Admission would suffice for casemix purposes because it is the best measure of the level of severity of the condition presented by the consumer to the treatment system.
9.1.2. In comparison, measurement of consumer outcomes by definition presumes a comparison over time and requires data to be collected on at least two occasions in order to allow assessment of change in the consumer’s health status.
9.1.3. The national protocol takes all these issues into account and requires that:
- clinical measures that are to be used for outcomes evaluation and casemix purposes be collected at the Admission, Review and Discharge Collection Occasions within episodes to allow change in the consumer’s clinical status to be assessed; and
- items required only for casemix purposes be collected at points which are consistent with the MH-CASC classification to allow the classification to be further developed. In general, the decision about whether to collect these at episode start or episode end is based on using the Collection Occasion that best describes the consumer during the overall episode of care.
9.1.4. As noted earlier, there were several recommendations from the NOCC Strategic Directions 2014-2024 project regarding revisions to the NOCC collection protocol, particularly with respect to the data requirements at closure of mental health care episodes in ambulatory settings.
9.1.5. The NOCC data requirements at discharge from ambulatory care are dependent on the reason for collection based on two broad considerations:
- Whether the care of the consumer is transferred from the ambulatory service to an inpatient or residential service of the same Mental Health Service Organisation; or
- Whether the duration of the ambulatory episode of mental health care was brief, as defined as an episode of care 14 days or less in duration (i.e., the number of days from admission to and discharge from the NOCC Ambulatory episode).
9.1.6. With respect to these two kinds of ambulatory discharge (i.e., transfer to bed- based care or brief episodes of care):
- the NOCC clinician and consumer-rated measures (i.e., the HoNOS/CA/65+, LSP-16, FIHS, the SDQ, BASIS-32/K-10/MHI-38) are not collected; and
- Mental Health Legal Status and Principal and Additional Diagnoses pertaining to the ambulatory episode are to be reported.
9.1.7. Regardless of whether the NOCC ambulatory episode of mental health care is closed either as a transfer or a brief episode as described in 9.1.5, a NOCC Discharge Collection Occasion must be recorded.
9.1.8. For both consumers and providers, the transition of treatment from ambulatory to bed-based care is a critical point in the delivery of services and therefore it is important to gain an understanding of the status of consumers and the outcomes of services provided. Where ambulatory discharge results in transfer to bed based care (i.e., an inpatient or community residential service of that Mental Health Service Organisation), wherever possible, the common clinician and consumer measure ratings for the admission NOCC in the inpatient unit or the residential care setting should be linked to the consumers’ discharge from the ambulatory episode.
Fig. 9.1 brings together these considerations and provides summary details of the various measures to be reported at the three Collection Occasions during each episode of mental health care.
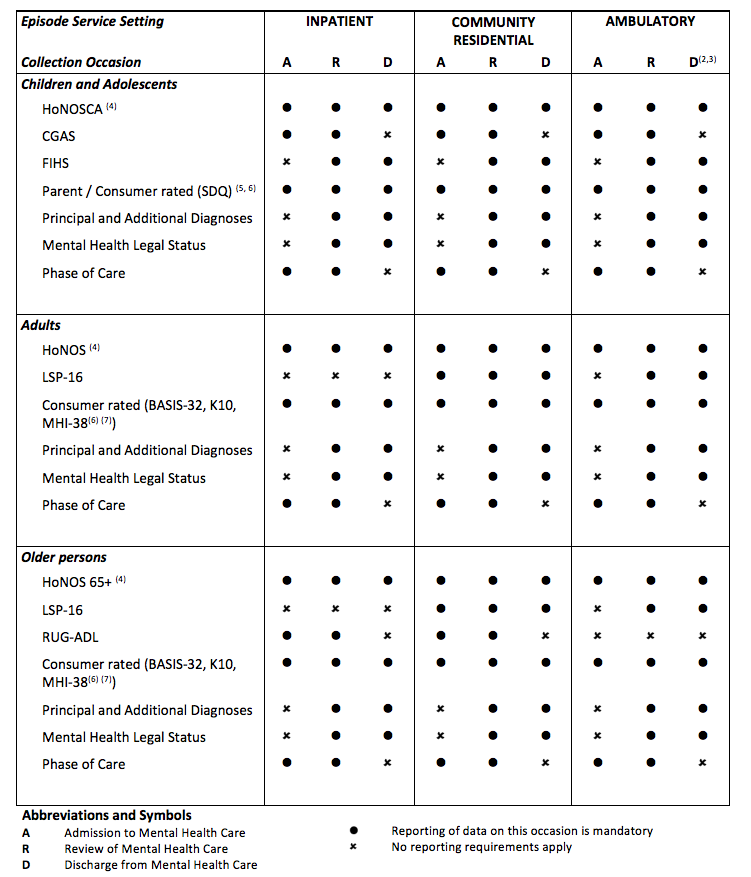
Fig. 9.1 Data to be reported at each Collection Occasion within each Episode Service Setting, for consumers in each Age Group
Notes
- This table identifies the national reporting requirements and is not intended to restrict a State or Territory from the collection of additional data at specific collection occasions.
- Discharge ratings for the clinician and consumer-rated measures (i.e., the HoNOS/CA/65+,LSP-16, FIHS, the SDQ, BASIS-32/K10/MHI-38) are not required by the ambulatory service or the consumer respectively, when the reason for the closure of the ambulatory episode is transfer to a bed-based treatment service setting of that organisation (i.e., psychiatric inpatient or community residential service). Where possible, the clinician and consumer measure ratings for the admission NOCC in the inpatient unit or the community residential care setting are reported as the consumer’s discharge ratings from the ambulatory episode. Details are required, however, regarding Principal and Additional Diagnoses and Mental Health Legal Status relevant to the ambulatory episode of care.
- Discharge ratings for the clinician and consumer-rated measures (i.e., the HoNOS/CA/65+, LSP-16, FIHS, the SDQ, BASIS-32/K10/MHI-38) are not required for brief ambulatory episodes. Brief ambulatory episodes are those where the number of days between admission to and discharge from the episode of care is 14 days or less duration. Details are required, however, regarding Principal and Additional Diagnoses and Mental Health Legal Status relevant to the ambulatory episode of care.
- Discharge ratings for the HoNOS, HoNOS65+ and HoNOSCA are not required for inpatient episodes of 3 days or less duration.
- Discharge ratings for the SDQ are not required for any episode of less than 21 days duration because the rating period used at discharge (previous month) would overlap significantly with the period rated at admission.
- The classification of consumer rated measures as mandatory is intended only to indicate the expectation that consumers will be offered to complete self-report measures at the specified Collection Occasions. There are circumstances where offering such measures will not be appropriate and special considerations applying to the collection of consumer rated measures are described in Special considerations applying to the collection of consumer self-report and parent measures.
- The K10L3D is a variation of the K10 designed for use in inpatient settings where the episode is of less than 3 days duration.
9.2. Rating periods for the clinical and consumer self-report measures and data items¶
Completion of each of the clinical measures and data items is based on a period of observation that is specific to each scale or item, and may vary according to the Collection Occasion. Table 9.1 identifies the usual rating periods and their exceptions for all clinical data. It should be noted that this Table refers only to the rating period and not to other criteria such as those relevant to the closure of Ambulatory Episodes as a result of transfer to an inpatient/residential setting or brief duration.
| Standardised measure or Data item | Usual rating period | Exceptions |
|---|---|---|
| HoNOS / HoNOS 65+ / HoNOSCA | Previous 2 weeks | At discharge from Inpatient psychiatric care, based on previous 3 days including day of discharge. |
| LSP | Previous 3 months | No exceptions |
| RUG-ADL | Current status | No exceptions |
| K10 / K10+ | For K10+LM, based on previous 4 weeks. For K10L3D, based on previous 3 days. |
No exceptions |
| BASIS-32 | Previous 2 weeks | No exceptions |
| MHI-38 | Previous 4 weeks | No exceptions |
| CGAS | Previous 2 weeks | No exceptions |
| FIHS | The period of care bound by the current Collection Occasion and the preceding Collection Occasion. | No exceptions |
| SDQ | At admission to a service, the previous six months At review and discharge, the previous one month |
No exceptions |
| PoC | There is no set rating period for PoC. PoC changes when there is a clinical decision that the primary goal of care has changed and there is a concomitant change to the mental health care plan. | No exceptions |
| Principal and Additional Diagnoses | The period of care bound by the current Collection Occasion and the preceding Collection Occasion. | No exceptions |
| Mental Health Legal Status | The period of care bound by the current Collection Occasion and the preceding Collection Occasion. | No exceptions |
Note
The K10L3D is a variation of the K10 designed for use in inpatient settings where the episode is of less than 3 days duration.
9.3. Special issues in interpreting the protocol at service delivery level¶
9.3.1. The standard protocol is designed to fit most clinical situations without there being an expectation that the fit will be perfect. Based on experience to date, it is expected that implementation of the protocol for the majority of cases should be relatively straightforward once information systems are in place and clinician training in use of the instruments has been completed.
9.3.2. However, there is a range of special issues that will need to be resolved within each jurisdiction where application of the standard protocol is more complex. Most of these concern clarifying the interface between episodes in complex sequences of care and interpreting the two business rules which act as triggers to data collection (one episode at a time, change of setting = new episode).
9.3.3. It is beyond the scope of the current document to provide detailed guidelines on all potential complexities arising in the translation of the standard protocol to the many service delivery environments in which mental health services operate in Australia. However, a summary of the approach recommended to the main issues is provided in Table 9.2 as a basis for further discussion within States and Territories and development of workforce training programs.
| Scenario | Common Questions | National minimum requirement |
|---|---|---|
|
Do NOCC clinical and consumer ratings need to be recorded for the end of the ambulatory episode as well as the beginning of the inpatient / residential episode when a consumer is transferred from ambulatory care to bed-based care? | Discharge ratings for the clinician and consumer-rated measures are not required by the ambulatory service or the consumer respectively, when the reason for the closure of the ambulatory episode is transfer to psychiatric inpatient or community residential care. |
|
Is the transfer of a patient from one psychiatric ward to another within the same hospital campus a new episode and thus requiring new data collection? | No, because there has not been a change of treatment setting. However, there may be good clinical reasons to reassess the patient when transfer occurs eg, when the transfer is from an acute to a rehabilitation ward, or from a general acute unit to a forensic ward within the hospital. Decisions about whether such additional ratings are required need to be resolved at the local level. Where they do occur, they should be reported and Reason for Collection coded as ‘Review – Other’. |
|
Should a new inpatient episode be commenced when a consumer is transferred from one hospital to another within the same mental health care organisation? | Yes. Even though this is not technically a change in treatment setting, States and Territories have agreed that an inpatient episode should be recorded in these circumstances, with the associated data collection requirements. |
|
Does a new cycle of data collection begin when case management is transferred from one ambulatory care team to another within the same organisation? | No, within the national episode model the consumer is regarded as remaining within the same episode of care. However, as in the example (2) above, there may be good clinical reasons to reassess the patient when between-team transfer occurs. For example, transfer from crisis team to continuing care team. Decisions about whether such additional ratings are required need to be resolved at the local level. |
|
Is each team expected to complete ratings on the consumer? | No, the consumer is regarded as receiving only one episode of care at a time. Decisions about which team (or clinician) is responsible for completing the required ratings need to be at the local level. In general, this is expected to be the service unit that is principally responsible for providing treatment and care during the current Episode of Mental Health Care. |
|
Is each day of care a new inpatient episode, requiring a full set of ratings? | No. Definitions developed under the National Survey of Mental Health Services since 1994, and now replicated in NMDS – Mental Health Establishments, regard ‘intended same day admissions’ as a component of ambulatory care services. |
|
Does an inpatient episode continue when a patient is placed on extended leave but remains, legally, an inpatient? | This is a common but complex issue in mental health services. As a general rule, it is recommended that, for the purposes of the NOCC dataset, the inpatient episode is deemed to have ended when the patient is sent on leave and where there is no intention that he/she return for an overnight stay within the next 7 day period. |
|
Does a new inpatient episode begin when a patient returns to hospital after a period of extended leave? | This is the converse of the above. It is recommended that where an inpatient episode is deemed to have ended as a result of indefinite leave, and the patient returns unexpectedly, a new inpatient episode should be commenced. |
|
Are discharge ratings required for very brief inpatient episodes? | In general yes, but there are exceptions:
In both instances above, the exclusion is because the period that would be rated at discharge would overlap with the admission ratings. Apart from the above exceptions, all other aspects of the collection protocol are required at discharge from inpatient episodes. |
|
How should the 3 monthly (91 day) review ‘rule’ be applied in these cases? Does it mean that they will need to be seen more regularly? | No, definitely not, the collection protocol is intended to support good practice rather than dictate how services should be delivered. Where the needs of a consumer require that they be seen regularly but at greater than 3 monthly intervals, then reviews using the standard instruments should be conducted on the next appointment that occurs after 3 months have elapsed since the last collection occasion. |
|
Is a new episode of mental health inpatient care commenced when the person is admitted to a (non-mental health) medical ward for the primary purpose of mental health care? | No. This is a continuation of the ambulatory episode. It is recommended however that a review of the consumer be conducted at this stage. |
|
What is expected of C-L teams in terms of collection of the NOCC data? | Consultation liaison is explicitly included as in scope for collection when there is a face-to- face assessment, with clarification that episodes extending over 14 days or less do not require discharge outcome measures to be collected. Outcome measures are to be collected at admission for all face-face assessments, and are to be collected at discharge when the episode of care (defined by the elapsed days from admission to discharge) is greater than 14 days. |
9.4. Special considerations applying to the collection of consumer self-report and parent measures¶
9.4.1. In general, all consumers should be asked to complete self–report measures at the Collection Occasions indicated in Fig. 9.1. However, due to the nature and severity of their mental health or other problems, it is likely that some consumers should never be asked to complete self–report measures, others may not be able to complete the self–report measures at the scheduled occasion, whilst still others may sometimes find completion of the self–report measures to be difficult or stressful. Suggested criteria for defining the reasons why the collection of self–report measures would be contraindicated are outlined below.
9.4.2. In all cases, clinical judgement as to the appropriateness of inviting the consumer to complete the measures should be the determining factor at any given Collection Occasion. Where collection of consumer self–report measures is contraindicated, the reasons should be recorded.
9.4.3. Similar considerations also apply in relation to the parent version of the SDQ.
General exclusions
9.4.4. Some persons may not be able to complete the measures at any time and should not be asked to do so. A definitive list of circumstances in which a general exclusion applies is beyond the scope of this document but broadly it would include situations where:
- the person’s cognitive functioning is insufficient to enable understanding of the task as a result of an organic mental disorder or an intellectual disability;
- cultural, language and/or literacy issues make the measures inappropriate. [1]
Temporary contraindications
9.4.5. Under certain conditions, a consumer (or in the case of the SDQ a parent) may not be able to complete the measure at a specific Collection Occasion. Circumstances where it may be appropriate to refrain from inviting the person to complete the measure include:
- where the consumer’s current clinical state is of sufficient severity to make it unlikely that their responses to a self–report questionnaire could be obtained, or that if their responses were obtained it would be unlikely that they were a reasonable indication of person’s feelings and thoughts about their current emotional and behavioural problems and wellbeing;
- where an invitation to complete the measures is likely to be experienced as distressing or require a level of concentration and effort the person feels unable to give; or
- where consumers or parents in crisis are too distressed to complete the measure.
9.4.6. It is suggested that in these circumstances consumers and parents need not be invited to complete the measures. At all other times, an attempt should be made to obtain their responses.
9.4.7. In many cases, the severity of the person’s clinical state and the degree of family distress experienced will diminish with appropriate treatment and care. It is suggested that, if within a period of up to seven days following the Collection Occasion in an ambulatory care setting the consumer (or parent) is likely to be able to complete the measure then their responses should be sought at that time. Otherwise, no further attempt to administer the measure at that Collection Occasion should be made.
Special issues related to the Strengths and Difficulties Questionnaire versions
9.4.8. The SDQ has six versions currently specified for NOCC reporting: [2]
- Parent-report for children aged 04-10 on admission to a mental health care episode;
- Parent-report for children aged 04-10 on follow up contact (review and discharge);
- Parent-report for children and adolescents aged 11-17 on admission to a mental health care episode;
- Parent Report Measure for Youth aged 11-17 on follow up contact (review and discharge);
- Youth self-report measure (11-17) on admission to a mental health care episode; and
- Youth self-report measure (11-17) on follow up contact (review and discharge).
9.4.9. Generally, the ‘admission’ versions are administered on admission and rated over the standard rating period of six months and the ‘follow up’ versions are administered on review and discharge and rated over a one month period. However, for referral from another setting, to prevent duplication and undue burden on consumers and parents, the following guide is suggested:
| Transfer of care between an inpatient, community residential or ambulatory setting of a consumer currently under the active care of the Mental Health Service Organisation. | Admission SDQ - if Follow Up SDQ required at the end of referring treatment settings episode is neither completed nor provided by referring setting. Follow Up SDQ - if Follow Up SDQ is required at end of referring treatment settings episode has in fact been completed and provided by the referring setting. |
| Admission to a new inpatient, community residential or ambulatory episode of care for any reason other than defined above. | Admission SDQ - if Follow Up SDQ required at the end of referring treatment settings episode is neither completed nor provided by referring setting. Follow Up SDQ - if Follow Up SDQ required at end of referring treatment settings episode has not been completed or is not provided by the referring setting. |
9.4.10. The ‘admission’ versions are to be used on admission of a consumer who is a new referral – that is, they are not currently under the active care of the Mental Health Service Organisation.
9.5. Future development of the protocol¶
The original version of the National Outcomes and Casemix Collection was prepared from the research and development undertaken in the first decade of the National Mental Health Strategy and the experiences by jurisdictions in introducing standard outcome measurement into routine clinical practice.
Recognising that the NOCC protocol has been in place for 10 years, in 2013 the MHISSC commissioned the NOCC Strategic Directions 2014-2024 project. The Final Report from that project contained 25 recommendations, several of which were implemented through earlier versions of the NOCC Technical Specifications.
The remaining recommendations require further research and development work and consultation within the mental health sector, and taking into consideration the evolving information requirements of the mental health sector.
| [1] | Substantial development work is required in the future to address cultural issues in the use and interpretation of self-report outcome measures. See Appendix 3. |
| [2] | An additional four versions are available for use by Teachers but these are not included in the national protocol. Details of these versions however are provided in the document Mental Health National Outcomes and Casemix Collection: Overview of clinician rated and self-report measures, Version 1.50. Department of Health and Ageing, Canberra, 2003. |