5. Overview of the clinical data to be collected¶
The agreed national requirements for outcomes and casemix data were first outlined in broad terms in the publication, Mental Health Information Development: National Information Priorities and Strategies under the Second National Mental Health Plan 1998-2003 (First Edition June 1999).
The specific clinical data to be collected depend on the type of Episode of Mental Health Care (inpatient, ambulatory, residential), the Age Group of the consumer, the Episode Service Setting and the Reason for Collection. Each of these concepts is discussed later in this document along with details on how they influence specific reporting requirements.
Each of the standard clinical and consumer self-rated measures is subject to its own set of collection guidelines, documented in their respective glossaries. These are not included in the current document but have been compiled separately in a resource document. [1]
This section provides an overview of each of the clinical and consumer self-rated measures and data items included in the Mental Health National Outcomes and Casemix Collection.
5.1. Clinical data specific to adults and older people¶
5.1.1. Health of the Nation Outcome Scales (HoNOS & HoNOS65+)¶
The Health of the Nation Outcome Scales (HoNOS) is a 12 item clinician-rated measure designed by the Royal College of Psychiatrists specifically for use in the assessment of consumer outcomes in mental health services. Ratings are made by clinicians based on their assessment of the consumer. In completing their ratings, the clinician makes use of a glossary which details the meaning of each point on the scale being rated.
The 65+ variant of the HoNOS has been designed for use with adults aged older than 65 years. It consists of the same item set and is scored in the same way, however the accompanying glossary has been modified to better reflect the problems and symptoms likely to be encountered when rating older persons.
Key References
General adult version:
Wing J, Beevor A, Curtis R, Park S, Hadden S, Burns A (1998) Health of the Nation Outcome Scales (HoNOS). Research and development. British Journal of Psychiatry, 172, 11-18.
Wing J, Curtis R, Beevor A (1999) Health of the Nation Outcome Scales (HoNOS): Glossary for HoNOS score sheet. British Journal of Psychiatry, 174, 432–434.
Older persons version: [2]
Burns A, Beevor A, Lelliott P, Wing J, Blakey A, Orrell M, Mulinga J, Hadden S (1999) Health of the Nation Outcome Scales for Elderly People (HoNOS 65+). British Journal of Psychiatry, 174, 424-427.
Burns A, Beevor A, Lelliott P, Wing J, Blakey A, Orrell M, Mulinga J, Hadden S (1999) Health of the Nation Outcome Scales for Elderly People (HoNOS 65+): Glossary for HoNOS 65+ score sheet. British Journal of Psychiatry, 174, 435-438.
5.1.2. Abbreviated Life Skills Profile (LSP-16)¶
The original LSP was developed by a team of clinical researchers in Sydney (Rosen et al 1989, Parker et al 1991) and, prior to the introduction of the NOCC collection, was in fairly wide use in Australia as well as several other countries. It was designed to be a brief, specific and jargon free scale to assess a consumer’s abilities with respect to basic life skills. It is capable of being completed by family members and community housing members as well as professional staff.
The original form of the LSP consists of 39 items. Work undertaken as part of the Australian Mental Health Classification and Service Costs (MH-CASC) study saw the 39 items reduced to 16 by the original designers in consultation with the MH-CASC research team. This reduction in item number aimed to minimise the rating burden on clinicians when the measure is used in conjunction with the HoNOS. The abbreviated 16-item instrument is the version to be reported under the Mental Health National Outcomes and Casemix Collection.
Key references
Original 39 item version of the LSP:
Rosen A, Hadzi-Pavlovic D, Parker G (1989) The Life Skills Profile: A measure assessing function and disability in schizophrenia. Schizophrenia Bulletin, 1989, 325-337.
Parker G, Rosen A, Emdur N, Hadzi-Pavlov D (1991) The Life Skills Profile: Psychometric properties of a measure assessing function and disability in schizophrenia. Acta Psychiatrica Scandinavica, 83 145-152.
Trauer T, Duckmanton RA, Chiu E (1995) The Life Skills Profile: A study of its psychometric properties. Australian and New Zealand Journal of Psychiatry, 29, 492-499.
Reference for LSP-16 (abbreviated 16 item version):
Buckingham W, Burgess P, Solomon S, Pirkis J, Eagar K (1998) Developing a Casemix Classification for Mental Health Services. Volume 2: Resource Materials. Canberra: Commonwealth Department of Health and Family Services.
5.1.3. Resource Utilisation Groups – Activities of Daily Living (RUG-ADL)¶
Developed by Fries et al for the measurement of nursing dependency in skilled nursing facilities in the USA, the RUG-ADL measures ability with respect to ‘late loss’ activities – those activities that are likely to be lost last in life (eating, bed mobility, transferring and toileting). ‘Early loss’ activities (such as managing finances, social relationships, grooming) are included in the LSP. The RUG-ADL is widely used in Australian nursing homes and other aged care residential settings. The RUG-ADL comprises 4 items only and is usually completed by nursing staff.
Key reference
Fries BE, Schneider DP, et al (1994) Refining a casemix measure for nursing homes. Resource Utilisation Groups (RUG-III). Medical Care, 32, 668-685.
5.1.4. Consumer self-report outcome measure¶
While the original Information Priorities document released in 1999 proposed the national use of a specific self-report measure (the Mental Health Inventory – MHI), this was subsequently changed to allow States and Territories to introduce an ‘agreed’ alternative measure. This recognised that, at the time when the NOCC reporting arrangements were designed, limited Australian research had been undertaken on consumer rated measures to identify the most suitable measure for use routine use in service delivery.
Following consultations with consumers within their jurisdictions, States and Territories introduced one of the following:
- Mental Health Inventory (MHI-38);
- Behaviour and Symptoms Identification Scale (BASIS-32); or
- Kessler–10 Plus (K-10+).
Table 5.1. provides a summary of the consumer self-rated measure currently used with adult and older consumers within each of the States and Territories.
| Jurisdiction | Measure |
|---|---|
| Victoria | BASIS-32 |
| New South Wales | K10+ |
| Tasmania | BASIS-32 |
| Australian Capital Territory | BASIS 32 |
| Northern Territory | K10+ |
| South Australia | K10+ |
| Western Australia | K10+ |
| Queensland | MHI-38 |
5.1.4.1. Mental Health Inventory (MHI-38)¶
The Mental Health Inventory (MHI-38) was designed to measure general psychological distress and well-being in the RAND Health Insurance Experiment, a study designed to estimate the effects of different health care financing arrangements on the demand for services as well as on the health status of the patients in the study.
The full form contains 38 items. Each item includes a description of a particular symptom or state of mind. The MHI can be completed either as a self-report measure or as part of an interview.
Key references
Veit CT and Ware JE (1983) The structure of psychological distress and well-being in general populations. Journal of Consulting and Clinical Psychology, 51, 730-742.
Davies AR, Sherbourne CD, Peterson JR and Ware JE (1998) Scoring manual: Adult health status and patient satisfaction measures used in RAND’s Health Insurance Experiment. Santa Monica. RAND Corporation.
5.1.4.2. Behaviour and Symptom Identification Scale (BASIS-32)¶
The Behaviour and Symptom Identification Scale (BASIS-32) was developed in the early 1990’s by a team in the United States for use in outcome assessment. The BASIS-32 asks the consumer to respond to 32 questions that assess the extent to which the person has been experiencing difficulties on a range of dimensions.
Key references
Eisen SV, Dill, DL and Grob MC (1994) Reliability and validity of a brief patient-report instrument for psychiatric patient outcome evaluation. Hospital and Community Psychiatry, 45, 242-247.
Eisen SV, Dickey B and Sederer LI (2000) A self-report symptom and problem scale to increase inpatients’ involvement in treatment. Psychiatric Services, 51, 349-353.
5.1.4.3. Kessler 10 Plus (K10+)¶
Originally developed in 1992 by Kessler & Mroczek [3] for use in the United States National Health Interview Survey, the K10 is a ten-item self-report questionnaire designed to yield a global measure of ‘non-specific psychological distress’ based on questions about the level of nervousness, agitation, psychological fatigue and depression in the relevant rating period. The K10+ contains additional questions to assess functioning and related factors, and it is this instrument which is being used by four States and Territories (New South Wales, Western Australia, South Australia, Northern Territory) in the NOCC. Overall, the K10+ is an extremely brief symptoms and functioning measure, validated against diagnosis that is intended to be supplemented with additional measures of domains relevant to consumers.
Key references
Andrews et al (1998): Andrews G. Sanderson K. Beard J (1998) Burden of disease. Methods of calculating disability from mental disorder. British Journal of Psychiatry 1998;173:123-31.
Kessler R, Costello EJ, Merikangas KR, Ustun TB (2000) Psychiatric Epidemiology: Recent Advances and Future Directions Chapter 5 in Manderscheid R, Henderson MJ (2000) Mental Health, United States, 2000. Rockville MD: Substance Abuse & Mental Health Services Administration, www.mentalhealth.org/publications/allpubs/SMA01-3537/
Andrews G and Slade T (2001) Interpreting scores on the K10. Australian and New Zealand Journal of Public Health, 25, 494-497.
Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczec DK, Normand S, Walters EE (2002) Short screening scales to monitor population prevalence and trends in non-specific psychological distress. Psychological Medicine, 32(6): 959-976.
Kessler RC, Colpe LJ, Epstein JF, Groerer JC, Hiripi E, Howes MJ, Normnad SL, Manderscheid RW, Walters EE, Zasalvsky AM (2003) Screening for serious mental illness in the general population. Archives of General Psychiatry 2003: 60(2), 184-189.
Note: Additional resource material is being prepared by the Centre for Mental Health, New South Wales Health Department and will be made available to all States and Territories. See also http://www.health.nsw.gov.au/policy/cmh/mhoat
5.2. Clinical data specific to children and adolescents¶
5.2.1. Health of the Nation Outcome Scales for Children and Adolescents (HoNOSCA)¶
The Health of the Nation Outcome Scales for Children and Adolescents (HoNOSCA) is a 15 item clinician-rated measure modelled on the HoNOS and designed specifically for use in the assessment of child and adolescent consumer outcomes in mental health services. Ratings are made by clinicians based on their assessment of the patient. In completing their ratings, the clinician makes use of a specific glossary which details the meaning of each point on the scale being rated.
Key references
Gowers S, Harrington R, Whitton A, Lelliott P, Beevor A, Wing J, Jezzard R (1999a) Brief scale for measuring the outcomes of emotional and behavioural disorders in children: Health of the Nation Outcome Scales for Children and Adolescents (HoNOSCA). British Journal of Psychiatry, 174, 413-416.
Gowers S, Harrington R, Whitton A, Beevor A, Lelliott P, Jezzard R, Wing J (1999b) Health of the Nation Outcome Scales for Children and Adolescents (HoNOSCA): Glossary for HoNOSCA score sheet. British Journal of Psychiatry, 174, 428-433.
5.2.2. Children’s Global Assessment Scale (CGAS)¶
The CGAS was developed by Schaffer and colleagues at the Department of Psychiatry, Columbia University to provide a global measure of severity of disturbance in children and adolescents. Similar to the HoNOSCA, it is designed to reflect the lowest level of functioning for a child or adolescent during a specified period. The measure provides a single global rating only, on a scale of 1–100.
Key reference
Schaffer D, Gould MS, Brasic J, et al (1983) A children’s global assessment scale (CGAS). Archives of General Psychiatry, 40, 1228-1231.
5.2.3. Factors Influencing Health Status (FIHS)¶
The Factors Influencing Health Status (FIHS) measure is a checklist of seven ‘psychosocial complications’ based on the problems and issues identified in the chapter of ICD-10 regarding Factors Influencing Health Status. It is a simple checklist of the ICD factors, originally developed for use in the MH-CASC project.
Key reference
Buckingham W, Burgess P, Solomon S, Pirkis J, Eagar K (1998) Developing a Casemix Classification for Mental Health Services. Volume 2: Resource Materials. Canberra: Commonwealth Department of Health and Family Services.
5.2.4. Parent and Consumer self-report measure – the Strengths and Difficulties Questionnaire (SDQ)¶
The Strengths and Difficulties Questionnaire (SDQ) is a brief behavioural screening questionnaire designed for 4-17 year olds and developed by Goodman et al in the United Kingdom. It exists in several versions to meet the needs of researchers, clinicians and educationalists.
General documentation of the SDQ is available on the website: www.sdqinfo.com. [4]
Key references
Goodman, R. (1997) The Strengths and Difficulties Questionnaire: A Research Note. Journal of Child Psychology and Psychiatry, 38, 581-586
Goodman, R. Meltzer, H. & Bailey, V. (1998) The Strengths and Difficulties Questionnaire: A pilot study on the validity of the self-report version. European Child and Adolescent Psychiatry, 7, 125-130. (Abstract)
Goodman, R. & Scott, S. (1999) Comparing the Strengths and Difficulties Questionnaire and the Child Behavior Checklist: Is small beautiful? Journal of Abnormal Child Psychology, 27, 17-24.
Goodman, R. (1999) The extended version of the Strengths and Difficulties Questionnaire as a guide to child psychiatric caseness and consequent burden. Journal of Child Psychology and Psychiatry, 40,791-801.
Goodman, R (2001) Psychometric properties of the Strengths and Difficulties Questionnaire. Journal of the American Academy of Child and Adolescent Psychiatry, 40:11, November 2001.
5.3. Other clinical data common to all consumer groups¶
5.3.1. Principal and Additional Diagnoses¶
The Principal Diagnosis is the diagnosis established after study to be chiefly responsible for occasioning the patient or client’s care in the period of care preceding the Collection Occasion. Additional Diagnoses identify main secondary diagnoses that affected the person’s care during the period in terms of requiring therapeutic intervention, clinical evaluation, extended management, or increased care or monitoring. Up to two Additional Diagnoses may be recorded.
Both Principal Diagnosis and Additional Diagnosis are collected as part of the Admitted Patient Mental Health Care NMDS, and Principal Diagnosis (but not Additional Diagnosis) is included in the Community Mental Health Care NMDS. Nevertheless, both data items are incorporated in the NOCC because the NMDS definitions are not suitable for development of outcomes and casemix analysis. Specifically, the reporting under the Admitted Patient Mental Health Care NMDS is based on the total hospital episode, while the Community Mental Health Care NMDS requires the diagnosis at the point of each service contact.
Under the NOCC protocol, the diagnoses assigned to the consumer are based on the Period of Care preceding the Collection Occasion, that is, the interval between the current Collection Occasion and that immediately preceding it within the current Episode of Mental Health Care.
5.3.2. Mental Health Legal Status¶
This item is used to indicate whether the person was treated on an involuntary basis under the relevant State or Territory mental health legislation, at some point during the period preceding the Collection Occasion.
Like the diagnosis items, Mental Health Legal Status is also collected under the National Mental Health Minimum Data Set arrangements but also included in the NOCC requirements due to differences in the reporting period used as the basis for recording the data item.
5.3.3. Mental Health Phase of Care (PoC)¶
The Mental Health Phase of Care is a prospective description of the primary goal of care for a consumer at a point in time. While many factors can impact on the consumer’s mental health care plan, the mental health phase of care is intended to identify the primary goal of care by the treating professional(s) through engagement with the consumer.
Key reference
Independent Hospital Pricing Authority (2016) Australian Mental Health Care Classification: Mental health phase of care guide. Ver 1.2 https://www.ihpa.gov.au/publications/mental-health-phase-care-guide
5.4. Purpose of the clinical data¶
The standard measures will be used for the purpose of measuring consumer outcomes or casemix classification, or both.
Fig. 5.1 summarises the data to be collected across the various consumer groups and the purposes of collection. In general, many of the measures will be used for both casemix development and outcome evaluation purposes.
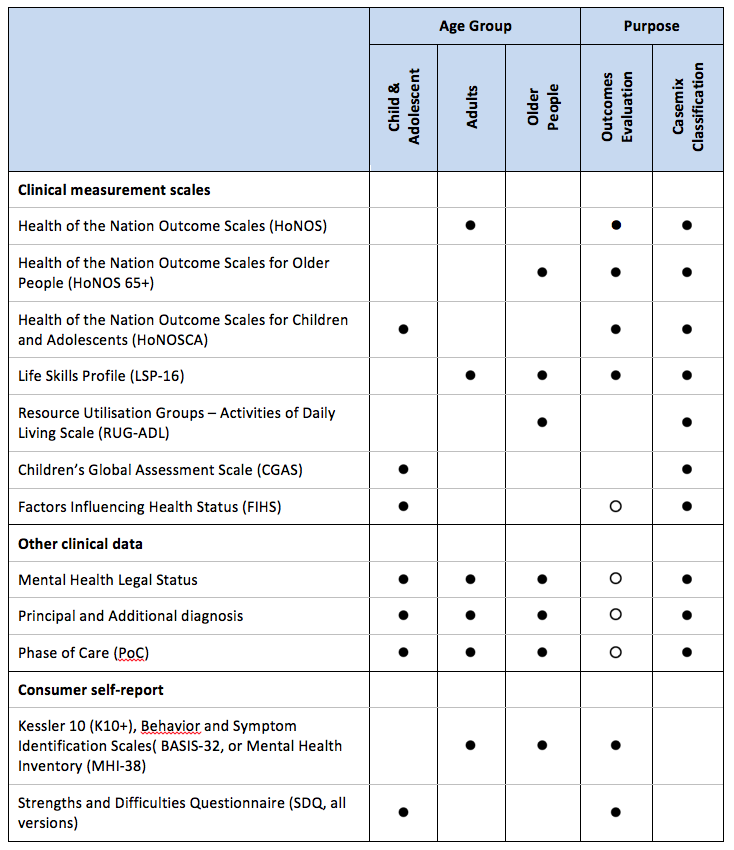
Fig. 5.1 Data to be collected and purpose of collection
Notes
Note: See also Fig.7.1 for details on when each of the above measures are to be collected.
Key to symbols
Solid bullet: Indicates the data will be used for the specified purpose of building the casemix classification or measuring outcomes.
While bullet: Indicates the data is not an outcomes measure as such but is important for the interpretation of outcome data.
| [1] | See Mental Health National Outcomes and Casemix Collection: Overview of clinical and consumer self-report measures and data items, Version 1.50. Commonwealth Department of Health and Ageing, Canberra 2003. |
| [2] | The version listed here is recommended for use in Australia. A newer version (the HoNOS 65+ Version 3, Tabulated) is published on the UK Royal College of Psychiatrists website at http://www.rcpsych.ac.uk/cru/honoscales/honos65/ but is not recommended for use at this stage due to non-comparability with the general adult HoNOS. |
| [3] | Kessler R, Mroczek D. Final versions of our Non-Specific Psychological Distress Scale. Ann Arbor MI: Survey Research Centre of the Institute for Social Research, University of Michigan, Memo dated March 10, 1994 |
| [4] | Please note that the versions labelled ‘English (Austral)’ currently on the SDQ website are not the versions specified for use in Australia. The versions for use in Australia can be found in the document: Mental Health National Outcomes and Casemix Collection: Overview of clinician rated and consumer self-report measures, Version 1.50. |